The Lancet has published today a really relevant ‘Viewpoint’ article:
Child undernutrition, tropical enteropathy, toilets, and handwashing by Dr
Jean Humphrey (of the Center for Human Nutrition, Johns Hopkins Bloomberg School of Public Health in Baltimore, MD and the
ZVITAMBO Project in Harare). The article starts off in a pleasingly forthright way:
Of the 555 million preschool children in developing countries, 32% are stunted and 20% are underweight. Child underweight or stunting causes about 20% of all mortality of children younger than 5 years of age and leads to long-term cognitive deficits, poorer performance in school and fewer years of completed schooling, and lower adult economic productivity.The hypothesis of the paper is simply:
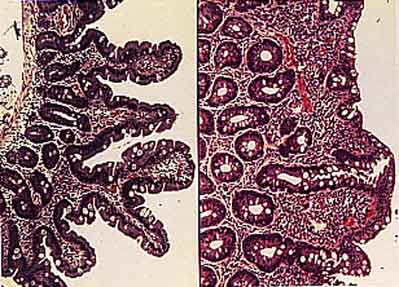
that a key cause of child undernutrition is a subclinical disorder of the small intestine known as tropical enteropathy, which is characterised by villous atrophy, crypt hyperplasia, increased permeability, inflammatory cell infiltrate, and modest malabsorption [details
here]
; that tropical enteropathy is caused by faecal bacteria ingested in large quantities by young children living in conditions of poor sanitation and hygiene; that provision of toilets and promotion of handwashing after faecal contact could reduce or prevent tropical enteropathy and its adverse effects on growth; and that the primary causal pathway from poor sanitation and hygiene to undernutrition is tropical enteropathy and not diarrhoea [emphasis added].
Dr Humphrey concludes her Viewpoint with:
Undoubtedly, the complex problem of child undernutrition will not be solved with toilets and handwashing alone. Interventions focused on gut microbial populations and improved drinking water quality might be important, together with continued efforts to improve infant diets. However, I hypothesise that prevention of tropical enteropathy, which afflicts almost all children in the developing world, will be crucial to normalise child growth, and that this will not be possible without provision of toilets. Randomised controlled trials of toilet provision and handwashing promotion that include tropical enteropathy and child growth as outcomes will give valuable evidence for this premise, and might offer a solution to the intractable problem of child undernutrition [emphasis added].
The African Report on Child Wellbeing: 2008 has some relevant quotes (the whole report is excellent − I’d not come across it before yesterday: it’s really quite disturbing):
Despite some progress, life for millions of Africa’s children remains short, poor, insecure and violent (page 90),
Too many children die needlessly before they reach the age of five, and too many have no access to health and medical services, adequate nutrition, safe water and improved sanitation services (page 11),
The best way of combating child death is to improve and expand access to primary health care, nutrition and improved water supplies, sanitation and hygiene – therefore to increase the budget allocated to public health (also page 11).
In August this year
The Lancet had an excellent ‘Comment’ article:
Child survival and IMCI: in need of sustained global support. Here’s a quote:
The broader determinants of child survival are crucial to understanding the potential effect of any set of interventions and the obstacles to reducing child mortality. An analysis of data from 152 countries [abstract
here]
noted that gross national income per head, female illiteracy, and income equality predicted 92% of the variance in child mortality. In low-income countries, where most child deaths occur, female illiteracy was more important than was gross national income per head, and both were more important than was public expenditure on health. A study from The Gambia [pdf
here]
showed that community and social networks, personal support for caregivers in the home, and financial autonomy were more important determinants of child mortality than was access to health services. Improvement of the quality of care in primary health clinics and referral hospitals will be essential to increase child survival, but as Arifeen and colleagues’ study [abstract
here]
shows, these interventions alone will be insufficient. Improvement of education of girls, social supports and networks for parents, economic equity, and sustaining broad-based maternal and child health services are all parts of what is necessary to reach targets for Millennium Development Goal 4. [MDG4 is to ‘Reduce child mortality’ − 2008 UN fact sheet
here].
So the message: clean up the environment, especially the immediate domestic and peri-domestic environment, by the provision and sustained use of sanitation and handwashing facilities, educate girls, and put public health right up very high on the political agenda. Fingers crossed − it could just work, especially if politicians, civil servants and local-government employees were to get off their asses and on with their job.
And here’s a brilliant quote from the paper
International Efforts to Control Infectious Diseases, 1851 to the Present (published in the Journal of the American Medical Association in September 2004):
Public health is ... an investment that works best when purchased in advance rather than paid out as each crisis arises.Quite. But the trick is to get those politicians to understand this, and understand it fully.
I’m indebted to the authors of the April 2009 World Bank Policy Research Working Paper No. 4907
How Can Donors Help Build Global Public Goods in Health? for this quote. This policy paper is very well worth reading in its own right − here’s its Abstract:
Aid to developing countries has largely neglected the population-wide health services that are core to communicable disease control in the developed world. These mostly non-clinical services generate “pure public goods” by reducing everyone’s exposure to disease through measures such as implementing health and sanitary regulations. They complement the clinical preventive and treatment services which are the donors’ main focus. Their neglect is manifested, for example, in a lack of coherent public health regulations in countries where donors have long been active, facilitating the spread of diseases such as avian flu. These services can be inexpensive, and dramatically reduce health inequalities. Sri Lanka spends less than 0.2% of GDP on its well designed population-wide services, which contribute to the country’s high levels of health equity and life expectancy despite low GDP per head and civil war. Evidence abounds on the negative externalities of weak population-wide health services. Global public health security cannot be assured without building strong national population-wide health systems to reduce the potential for communicable diseases to spread within and beyond their borders. Donors need greater clarity about what constitutes a strong public health system, and how to build them. The paper discusses gaps in donors’ approaches and first steps toward closing them.[The only thing I’d add is that many, if not most, developing-country governments also “need greater clarity about what constitutes a strong public health system, and how to build them”, not just donors.]
And it starts with another good quote:
Focusing on clinical services while neglecting services that reduce exposure to disease is like mopping up the floor continuously while leaving the tap running.





{kind=link}